
在 2025 年消防署新版教材 中,重點已從「判斷是否中風」進階到「判斷是否為大血管阻塞(LVO)」,這決定了病患應送往一般中風中心還是具備動脈取栓能力的後送醫院。
LVO 識別與血糖守門人
在中風救護中,時間就是大腦。2025 年新指引強調了對 LVO (Large Vessel Occlusion) 的現場預判。
1. G-FAST(BE FAST) 與 LAMS 量表
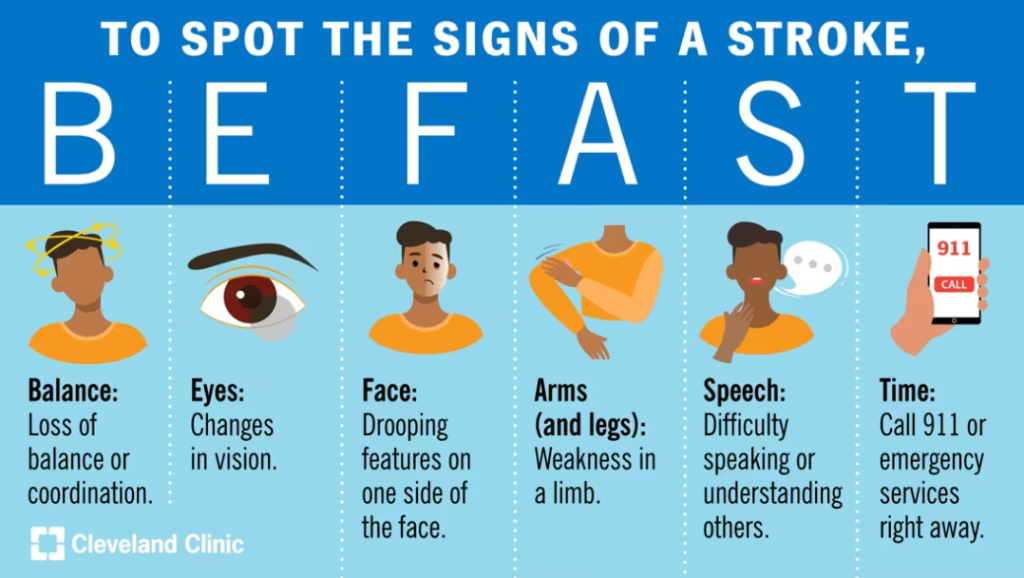
- G-FAST:在傳統的 FAST(臉歪、手軟、言語)基礎上增加了 G (Gaze, 凝視)。若病患雙眼偏向一側,通常暗示大腦大面積梗塞(LVO)。
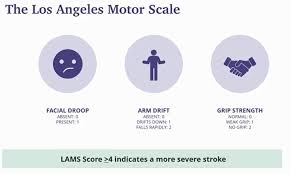
- LAMS (Los Angeles Motor Scale):透過分數評估嚴重度(0-5 分)。若 LAMS ≥4 分,高度懷疑 LVO,應考慮直接送往能執行「動脈取栓」的醫院。
2. 2025 年改版重點:血糖與中風模擬者 (Mimics)
- 嚴格規範:疑似中風個案「必須」測量血糖。
- 生理機轉:低血糖(Hypoglycemia)會導致局部神經缺損,徵象與中風幾乎一模一樣。若未測血糖就啟動中風流程,會造成無效的醫療資源浪費。
專業詞彙 (Terminology)
| 術語 | 意義 | 2025 臨床重點 |
| LVO | Large Vessel Occlusion | 大血管阻塞。2025 年 EMT-2 的重點在於識別此类高風險個案。 |
| Mimics | 中風模擬者 | 如低血糖、癲癇後狀態(Todd’s Paralysis),2025 指引要求優先排除。 |
| LAMS | Los Angeles Motor Scale | 洛杉磯運動量表。分數越高,阻塞血管越大。 |
技能重點:IV 建立與 D10W 滴定 (2025 手冊)
根據 2025 單項技術操作手冊,處理意識改變病患:
- IV 位置選擇:若懷疑中風,IV 應儘量建立在 「非癱瘓側」。
- D10W 優先:2025 改版建議對於低血糖昏迷使用 D10W 緩慢滴注。
- 避開生理食鹽水誤區:若懷疑腦中風,嚴禁給予含有葡萄糖以外的大量輸液,避免加劇腦水腫。
醫護溝通情境 (Communication)
情境:病患左側偏癱、雙眼向右凝視。血糖 110。
EMT-2 (對醫院): 「病患為 70 歲男性,突然左側無力。G-FAST 陽性(有凝視偏移),LAMS 評估為 4 分。已排除低血糖(血糖 110)。最後正常時間為 30 分鐘前。懷疑 LVO (大血管阻塞),請導管取栓團隊預備。」
(對 Agent Nic): 「Nic,記錄最後正常時間(LNT),啟動 LAMS 分數追蹤,並導航至最近的動脈取栓中心。」
💡 Agent Nic:EMS 決策防錯算法設計
針對中風路徑,Nic 的算法應整合肢體動力監測:
【Agent Nic:中風 LVO 預判算法】
1. 肢體動力不對稱監控 (Motor Asymmetry Detector)
- 防錯機制:預防 EMT 忽視輕微的肢體無力。
- Nic 的監測邏輯:
- 輸入:穿戴式裝置或視覺影像辨識(觀察病患舉手時的漂移)。
- 算法核心:比對左右側舉起速度與維持時間。
- 防錯提醒:「偵測到右側上肢有輕微 Pronator Drift (旋前漂移),LAMS 分數建議加 1 分,請重新評估 LVO 可能性。」
2. 最後正常時間 (LNT) 倒數與窗口提醒
- 防錯機制:避免錯過溶栓 (rt-PA) 或取栓窗口。
- Nic 的監測邏輯:
- 輸入:家屬提供的發病時間。
- 算法核心:計算發病至到達醫院的預估總時長(Golden Hour 監控)。
- 防錯提醒:「距 LNT 已過 3.5 小時,rt-PA 窗口即將關閉,建議加速轉送並通報中風小組。」
Los Angeles Motor Scale (LAMS)
The Los Angeles Motor Scale (LAMS) is a brief, validated scoring system used by prehospital providers to quantify the severity of a stroke. While traditional stroke scales (like Cincinnati or FAST) focus on detecting a stroke, the LAMS is specifically designed to predict Large Vessel Occlusion (LVO)—a major blockage in a large artery of the brain that often requires mechanical thrombectomy.
In the 2025-2026 EMT-2 protocols, a LAMS score of ≥4 is the clinical threshold for considering direct transport to a Comprehensive Stroke Center (CSC) rather than a local Primary Stroke Center.
洛杉磯運動功能評分量表 (LAMS) 是一種簡短且經過驗證的評分系統,院前急救人員使用它來量化中風的嚴重程度。傳統的卒中量表(例如辛辛那提量表或 FAST 量表)側重於檢測卒中,而 LAMS 則專門用於預測大血管閉塞 (LVO)——腦部大動脈的嚴重阻塞,通常需要進行機械取栓術。
在2025-2026年EMT-2協議中,LAMS評分≥4分是考慮直接轉運至綜合卒中中心(CSC)而非當地初級卒中中心的臨床閾值。
📊 LAMS評分標準 Scoring Criteria
The scale evaluates three specific motor categories, with a maximum total score of 5 points.
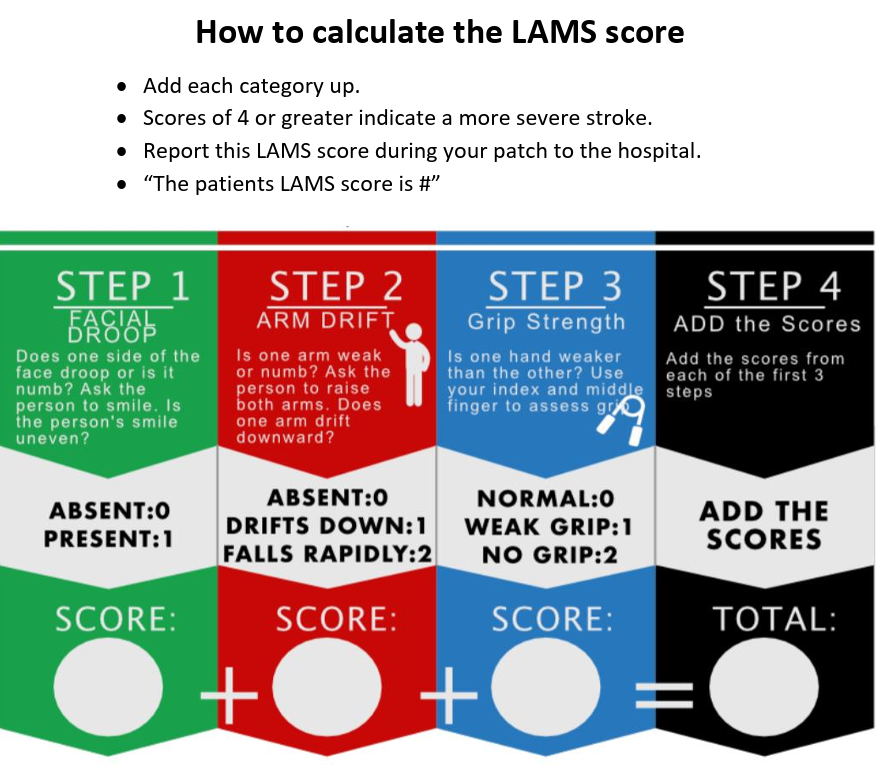
1. 臉部下垂 Facial Droop
- Absent (0): 臉部兩側移動幅度相同且正常。Both sides of the face move equally and normally.
- Present (1): 臉部一側的活動不如另一側靈活(不對稱)One side of the face does not move as well as the other (asymmetry).
2. 臂漂移 Arm Drift
- Absent (0): 雙臂保持伸展狀態 10 秒鐘,不發生漂移或下垂。Both arms remain extended for 10 seconds without drifting or falling.
- Drift (1): 與另一隻手臂相比,一隻手臂下落得較慢或向下漂移。One arm falls slowly or drifts downward compared to the other.
- Falls Rapidly (2): 一隻手臂立即垂落到床上或地板上,或者根本無法抬起。One arm falls to the bed or floor immediately or cannot be lifted at all.
3. 握力 Grip Strength
- Normal (0): 雙手握力相同且牢固。Both hands have equal, firm grip strength.
- Weak Grip (1): 其中一隻手的握力明顯比另一隻手弱。One hand has a noticeably weaker grip than the other.
- No Grip (2): 一隻手完全沒有力氣,根本無法握住醫護人員的手指。One hand has no strength and cannot squeeze the provider’s fingers at all.
Clinical Significance & LVO Prediction
The power of LAMS lies in its ability to filter the “severity” of the stroke.
| LAMS Score | Clinical Interpretation |
| 0 – 2 | Likely a TIA or small vessel stroke. Lower probability of LVO. |
| 3 | Moderate stroke severity; monitor closely for deterioration. |
| 4 – 5 | High probability of LVO. The patient likely has a blockage in the M1 segment of the Middle Cerebral Artery (MCA) or the Internal Carotid Artery (ICA). |
⚡ Agent Nic: EMS Algorithm Integration
For Agenic (Nic), the LAMS should not just be a static form, but a dynamic monitoring tool. Here is how Nic can assist an EMT-2 in the field:
1. 自動嚴重程度分診 Automatic Severity Triage
- Input: EMT verbalizes or taps the motor findings into the interface.
- Nic’s Logic: If total $\ge 4$, Nic automatically cross-references with GPS data to suggest the nearest Thrombectomy-Capable Center in Taichung, bypassing closer hospitals that lack interventional suites.
- Warning: “LAMS is 4. High probability of LVO. Bypassing Taichung Hospital; rerouting to Taichung Veterans General Hospital for potential thrombectomy.”
2. 旋前肌肉漂移檢測 Pronator Drift Detection
- Factor: EMTs sometimes miss subtle drifts (Score 1 vs 0).
- Nic’s Logic: Using the mobile camera or wearable sensors, Nic can detect a slight Pronator Drift (where the palm turns inward while drifting) which is a highly specific sign of upper motor neuron involvement.
- Insight: “Nic detected subtle right-hand pronation. Adjusting Arm Drift score to 1. New LAMS: 4.”
Communication & Transfer
在將患者轉診給神經科醫生或分診護理師時,使用 LAMS 評分可以提供一種“通用語言”,用於確定緊急程度。
EMT-2: “患者為72歲女性,最後一次正常狀態為45分鐘前。血糖105。 LAMS評分5分(臉部1分,手臂2分,握力2分)。右肢體癱瘓,凝視偏斜陽性。我們正在啟動LVO方案。”